

On the Impossibility of Making a Pie Chart of Client Problems
On the Impossibility of Making a Pie Chart of Client Problems
How's that for a mouthful?

The quotation I think about most when writing about mental health is from Anne Harrington’s Mind Fixers: Psychiatry's Troubled Search for the Biology of Mental Illness (2019):
...current brain science still has little understanding of the biological foundations of many—indeed most—everyday mental activities. This being the case, how could current psychiatry possibly expect to have a mature understanding of how such activities become disordered—and may possibly be reordered?1
I like this quote because it explains why mental health experts have little to no idea what they are doing. From psychologists to psychiatrists, from researchers to clinicians, and from theory to practice, current notions of psychological phenomena are for the most part well-intentioned and woefully arrogant. What else can we expect from a discipline that is essentially asked to perform magic?2
It’s not only the brain in isolation that science doesn’t understand, but how the brain interacts with other brains, novel environments (evolutionary mismatch), psychiatric medications, and so on. We don’t even really know how the brain, that lump of meat inside our skulls, relates to the mind, our conscious experience. “There is nothing that we know more intimately than conscious experience,” David Chalmers writes in Facing Up to the Problem of Consciousness, “but there is nothing that is harder to explain.” To think that someone could be endowed with enough knowledge of these mysteries to be even minimally effective in fixing mental illness, sometimes in the mere two years required for a master’s degree, is ridiculous. And yet this is the basic assumption that most people have of mental health professionals. Otherwise, we wouldn’t have installed them in every nook of our society.
Even a clinician who, I don’t know, spends around 20 hours a week studying and writing at the frontier of the best science available—nice to meet you—is mostly flying blind. For example, a friend asked me recently if I could make a pie chart of my clients’ problems, given that I’ve been seeing clients for nearly a decade. Because I’d tried this exercise before, I was ready with my answer: “No.”
Not meaningfully, at least. Sure, I could create broad categories such as relationships, work, health, and so on, but these wouldn’t be valuable (or interesting) because they wouldn’t usefully explain the cause of my clients’ suffering. Which relationship(s)? What about them?
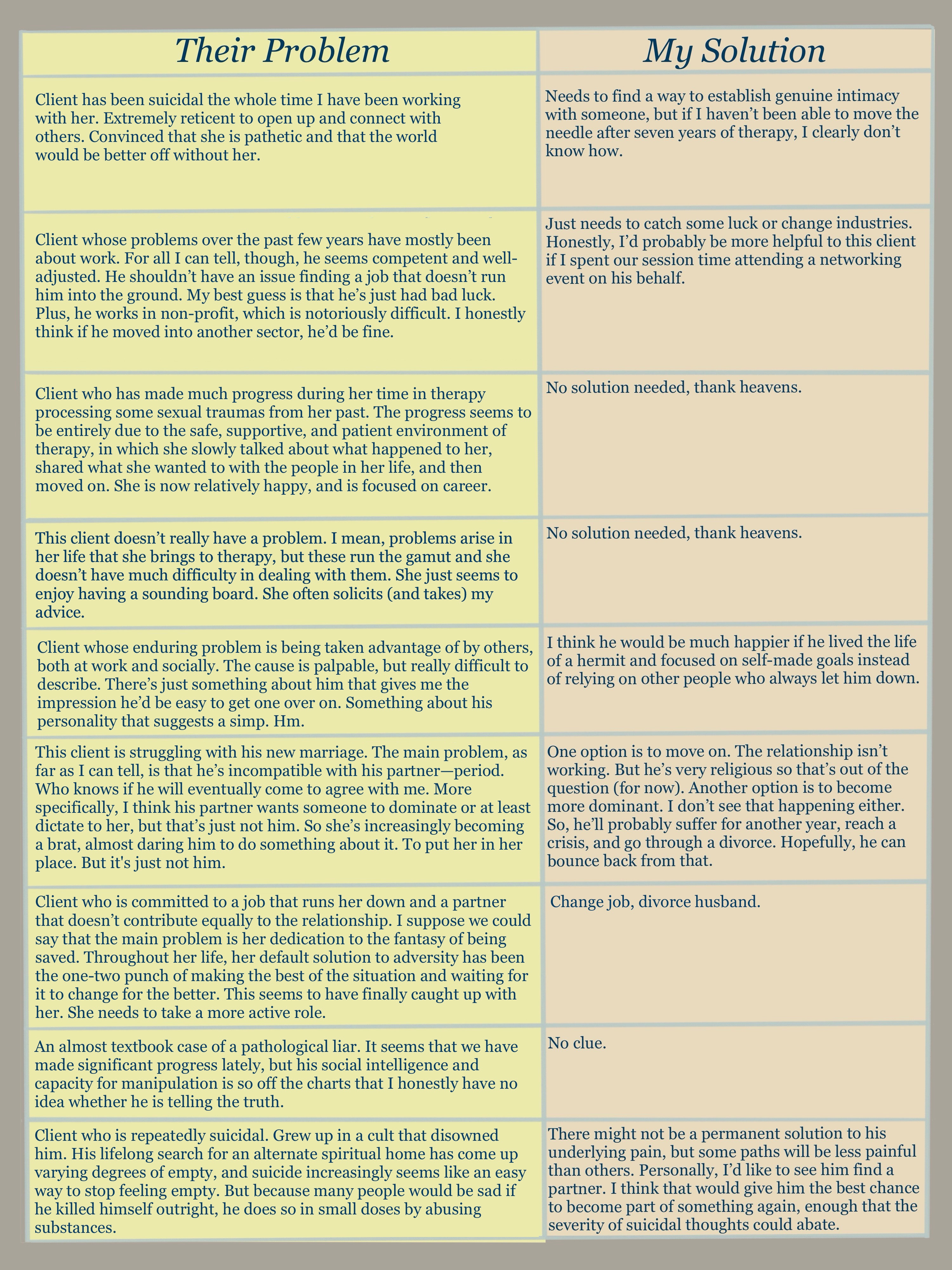
To appreciate how difficult it would be to make a meaningful pie chart, here are the problems of the last nine clients that I’ve seen, as simply as I can state them:3
Client has been suicidal the whole time I have been working with her. Extremely reticent to open up and connect with others. Convinced that she is pathetic and that the world would be better off without her.
Client whose problems over the past few years have mostly been about work. For all I can tell, though, he seems competent and well-adjusted. He shouldn’t have an issue finding a job that doesn’t run him into the ground. My best guess is that he’s just had bad luck. Plus, he works in non-profit, which is notoriously difficult. I honestly think if he moved into another sector, he’d be fine.
Client who has made much progress during her time in therapy processing some sexual traumas from her past. The progress seems to be entirely due to the safe, supportive, and patient environment of therapy, in which she slowly talked about what happened to her, shared what she wanted to with the people in her life, and then moved on. She is now relatively happy, and is focused on career.
This client doesn’t really have a problem. I mean, problems arise in her life that she brings to therapy, but these run the gamut and she doesn’t have much difficulty in dealing with them. She just seems to enjoy having a sounding board. She often solicits (and takes) my advice.
Client whose enduring problem is being taken advantage of by others, both at work and socially. The cause is palpable, but really difficult to describe. There’s just something about him that gives me the impression he’d be easy to get one over on. Something about his personality that suggests a simp. Hm.
This client is struggling with his new marriage. The main problem, as far as I can tell, is that he’s incompatible with his partner—period. Who knows if he will eventually come to agree with me. More specifically, I think his partner wants someone to dominate or at least dictate to her, but that’s just not him. So she’s increasingly becoming a brat, almost daring him to do something about it. To put her in her place. But it's just not him.
Client who is committed to a job that runs her down and a partner that doesn’t contribute equally to the relationship. I suppose we could say that the main problem is her dedication to the fantasy of being saved. Throughout her life, her default solution to adversity has been the one-two punch of making the best of the situation and waiting for it to change for the better. This seems to have finally caught up with her. She needs to take a more active role.
An almost textbook case of a pathological liar. It seems that we have made significant progress lately, but his social intelligence and capacity for manipulation is so off the charts that I honestly have no idea whether he is telling the truth.
Client who is repeatedly suicidal. Grew up in a cult that disowned him. His lifelong search for an alternate spiritual home has come up varying degrees of empty, and suicide increasingly seems like an easy way to stop feeling empty. But because many people would be sad if he killed himself outright, he does so in small doses by abusing substances.
Can you make a meaningful pie chart from the descriptions above? Seriously, if you can, let me know.
Of course, the standard way for categorizing client problems comes courtesy of The Diagnostic and Statistical Manual of Mental Disorders (DSM), which is sometimes called “the Bible of psychiatry.”4 The issue, as Allen Frances notes, is that:
All diagnoses…are purely descriptive—just names for symptoms that tend to go together…None…is the slightest bit explanatory—causes are too complex/interacting for us to understand.
Plus, even with over 300 disorders listed in the current edition, the DSM doesn’t have much to say about the cases I presented above, does it? Most of my clients don’t neatly fit the criteria for, say, bipolar disorder, schizophrenia, or post-traumatic stress disorder. Could I shoehorn some of them into a diagnosis for insurance reimbursement purposes? You bet your tax-paying dollars I could. But if we were hoping to make a meaningful pie chart using the standard clinical playbook, it’s not going to happen.5
“Tell me what you really think”
For the past eight years, then, my clients have asked me for help with problems that elude useful categorization, which is great for keeping my job fresh, but not very conducive to building expertise.6 And if you’re thinking, well, you sound like a generalist, but surely someone who specializes in eating disorders, for example, has a better handle on what they’re doing, my response would be—not really.
For example, this summary of eating disorders could apply in large strokes to dozens of other mental health conditions. The template is as follows:
We (the experts) don’t really know why [insert condition] develops, but we know it’s as a result of a complex interplay involving [insert every factor under the sun, e.g. genes, stress/trauma, family history, society, comorbidities, and so on].
A bunch of significantly different approaches have proven to be moderately effective for [insert condition]. We don’t quite know why these treatments are effective, or which will work best for you. So maybe try them all?
More research is needed to figure out something of actual value.
Hopefully, you are beginning to see what therapists are up against. When people look back from the vantage point of finally understanding the brain (if this day ever comes), they will pity today’s therapists for the absurdity of their task.
Let’s return to the list above. Here is my honest assessment of the solutions needed, to say nothing of the additional step of convincing the client to do them:
“Honey, I Shrunk the Problems”
So far, we’ve established that therapists have an impossible task—not that most of them know it—because of the variety of problems brought to their door and the lack of available knowledge about the ultimate driver of experience, the brain. I mean, I can’t even answer a friend’s simple and well-intentioned question about the kind of problems I’ve presumably been solving for close to a decade.
But it’s not just me and my practice. The opportunities for demonstrating how little clinical psychology knows are manifold. When psychiatric medication works, we don’t know why. Most of the therapeutic orientations work just as well as another, calling into question the principles that distinguish them. It’s also possible that in some cases, exercise is a better solution. In short, someone whose eye lingers for even a brief moment on the mental health industry is likely to raise an eyebrow.
Now, many of these complaints have been leveled at the field already, but one that I haven’t come across is that plenty of mental states result from subtle dynamics that, perhaps because of their subtlety, the clinical community doesn’t talk about. Just last week, three clients described experiences for which there is pretty much zero therapeutic acknowledgement, that I nevertheless understood deeply. The lack of discussion about these fine-grained antecedents to our mental states is a further handicap on the field’s ability to help.
First, Josiah talked about the pleasures of a shrunken world. Having quit his job recently, he has far fewer responsibilities, and no need to travel more than ten minutes from his home. So much of his happiness, we are coming to discover, is remaining under a certain stimulus threshold. His daily trek to the city, what with the sights, smells, and sounds—to say nothing of the running-around at work—was simply too much for someone who is, at base, more sensitive to the average stimulus than most. But this general dynamic applies to everyone, and we could say broadly that if people’s lives don’t fall into an acceptable “stimulus band” set largely by their genes, they are going to be perpetually agitated or bored. (Bigger words for which, by the way, might be anxious or depressed.) Yet this “stimulus band” perspective is hardly mentioned in therapeutic circles.
Second, Mishara has been talking to me for months about the aesthetics of her neighborhood. She spends much of her time volunteering for clean-up and “block beautification” projects. I, too, often lament how ugly the scene is out my window, and wonder what sort of effect that has on my view of the world. Yet clinical psychology rarely, if ever, mentions the importance of beautiful surroundings. I mean, there is some literature on the effect of green spaces on anxiety and crime, but by and large, the ability to see pleasant stuff—or at least not see ugly stuff—is low on the priority list. A clinical training program would never create a fake client with this kind of problem.
I think our vantage point, though, can matter a great deal. This is something that was brought home to me by a third client, Winston, who often expresses his love for the desert landscape. “Simple, unending, clean.” He says that since moving East, he’s noticed a certain claustrophobia in cities and wooded areas. He pines (no pun intended) for vast, open spaces, where he can think much better. Again, these are difficult dynamics to pin down, but I have little trouble understanding them because I feel many of them myself. I mean, you’d be shocked by how much of my current happiness I attribute to being on the top floor of my apartment complex. Not only does this eliminate the possibility of upstairs neighbors ruining my day, but I also enjoy having the high ground. To some primal instinct of mine, being above others signals that I am safe. I can relax.
For every time the mental health industry doubles down on the big-ticket items like “anxiety and depression,” someone is having a “smaller,” but nevertheless distinct and relatable, feeling that lacks representation, which subsequently makes it difficult or even embarrassing to describe. In all my reading and training in mental health, I’ve never come across any of the dynamics above, but obviously they are important if multiple clients discuss them and I understand them. Yet another example of how much more ground clinical psychology has to cover…
The good news is that much of it has already been covered—not by clinical psychologists, but by artists. Artists have run circles around the scientific community when it comes to the finer points of human experience, and because of this, something like reading literature would be a better preparation for prospective therapists than a clinical training program.7 To write convincing characters, novelists and playwrights have to have a very deep understanding of human nature. But anyone can get a degree in counseling or psychology if they just sit around long enough.
Sate Expectations
The large blank space in humans’ knowledge of their own brain should, in my opinion, cause mental health professionals to reduce their ambitions. To curtail their authority. As a society, I think the default assumption should be that therapists are a special kind of friend or guide, and that therapy is a unique kind of space in which to have a conversation. Therapists shouldn’t be considered doctors of the mind, because they aren’t. They don’t have enough knowledge, or proven technique, to make that claim, to hold themselves out as such.8
Early in my training, my supervisor would tell me: “As long as the client is talking, you’re doing your job.” Not only did this relax me, but it also helped reset my expectations. My job isn’t to fix clients, because usually I can’t. Most of the time, there’s nothing I can do but listen and support. Often, that is all the client wants. In the remaining cases, though, in which clients want more than I can provide…that is where a cultural realignment, with respect to what therapists can realistically accomplish, would be helpful. Remember, perception is the result of outcomes minus expectations, and if the expectation is that therapy is magic, plenty of people will be disappointed.
Our understanding of the value of therapy should not depend on the special knowledge or abilities of the therapist unless that knowledge and those abilities are about having a meaningful conversation. The therapist is neither doctor nor magician. They are simply another person, often stuffed with just enough knowledge to be dangerous, whose salvation lies in their intention and position. My main value is that I genuinely care about my clients and am not a part of their lives. This allows them to open up for forty-five minutes at a time—an eternity in a shared conversation—about a wider range of topics than they would elsewhere.
That, right there, accounts for the bulk of therapy’s benefit. If society wants more from therapy and therapists, it will simply have to wait.
p. 276, emphasis original.
This arrogance might be amplified by the fact that the entity in question is the human brain, with whose workings we imagine we are familiar.
Some of the information has been scrambled to protect client identity, but not the core of the problem.
Presumably because it’s just as scientific.
You might also be surprised that a fair number of my clients aren’t experiencing “major” problems. But considering that only about 1% of the population has what is called “severe mental illness” (SMI), this is pretty typical for the average caseload.
I hope to write a post soon on clinical training, but the tl;dr is that it’s bad. Real bad.
Neither do psychiatrists: “Psychiatry has at least one possible alternative, but it would require an act of great professional and ethical courage. It could decide to return to a less hierarchical understanding of its place in the mental health and medical systems; one that...would acknowledge that mental suffering is a larger category than mental illness, and that even disorders with a likely or possible biological basis are not just medical, because the experiences of all human beings, ill or otherwise, are shaped by their cultural, social, and familial circumstances.” – Mind Fixers, p. 273-274, emphasis original.
Given all this uncertainty, I have a question -- hopefully one that won´t come off as glib or unduly critical of your profession. Why get therapy? Of course some people want to and have the funds to do so, and in this case I totally get it. But what about the people who don´t want to?
I´m thinking of a specific case: my partner. He´s been diagnosed with schizoaffective disorder and his sessions regularly cause him anxiety. Just the process of getting on the bus to go to his therapists office is a stress. He says "everybody has problems so why am I the only one who has to go to therapy?" (Good point.) He says "she´s already told me what to do and now I just have to do it but it´s hard." (Good point.) Bottom line, he doesn´t want to go but his psychiatrist says he needs to. Given the expense and uncertainty about whether it would even work, should he be cajoled into going?
I´m kind of asking for free advise here so feel free not to answer if you´d rather not. Just thought I´d share what came up for me after reading your post. Thanks!
Jesus Christ.